
Article
Top 10 SaMD Job Boards & Regional Organizations

This is Part 1 of the two-part interview between Orthogonal’s Randy Horton and Francesca Wuttke and Xenia Riasol of nen.
Links to individual parts of the interview:
When Francesca Wuttke struck out to develop a groundbreaking and viable Digital Therapeutic (DTx) solution to address an underserved population, she could think of no better partner than Xenia Riasol. The former coworkers bring their long-time healthcare, startup acceleration and Digital Therapeutic expertise to nen, a novel digital solution that uses Cognitive Behavioral Therapy (CBT) to help children with cancer manage their pediatric oncology pain.
Randy Horton, Orthogonal’s VP of Partnerships, sat down with Francesca and Xenia to discuss all things nen. Between landing interest and funding for their early stage startup, to gathering clinical experts to advise the creation of their DTx, Francesca and Xenia paint a picture of nen’s potential to transform the lives of kids with cancer.
In Part 1 of this interview, Francesca and Xenia discuss their backgrounds, the origins of nen and its mission statement and how they leveraged their large professional networks to get in touch with eager supporters, investors and clinical experts.
Randy:
Good morning, Francesca and Xenia. Thanks for joining me today. This is a great opportunity to hear from two very seasoned people in digital health and Digital Therapeutics, who are now at the very beginning of their journey with their own startup.
Could you start by giving a little background on yourselves and how you got into the Digital Therapeutics space?
Francesca:

I’m Francesca Wuttke, the founder and CEO of nen. I have over 25 years of drug development and healthcare expertise in both the U.S. and Europe. I’ve worked with diverse organizations including startups, consultancies – including one I ran for a while in New York – large and specialty pharma and academia. I started my career in clinical trial management and trained as a scientist. I anticipated working on HIV drug design, but I moved to private equity – as you do. Eventually I went to Big Pharma. I started at Novartis in a development strategy role, and moved to a commercial strategy role within the newly minted cell and gene therapy group. I was responsible for innovating on commercial strategy and bringing in new products to the pipeline.
My family made the decision to move to Barcelona. There, I joined Almirall as part of their corporate development group, leading strategy for the organization. Then I moved to MSD Global Health InnovationFund, LLC, a $500,000 venture capital fund dedicated exclusively to digital health and health-enabling technology investments, where my focus was on software-enabled clinical trial solutions. Eventually I went back to Almirall and became the Chief Digital Officer, responsible for the end-to-end digital transformation of the company: everything from back office process automation to data analytics and DTx. I met Xenia at Almirall. We worked together to create the Digital Garden, an in-house startup accelerator for digital health innovators. Between the Digital Garden and the projects that we ran, we collaborated with over 27 startups. I think I’ve evaluated over 1,000 business models and pitch decks.
Randy:
And this is your first startup. It’s your baby from the start.
Francesca:
It’s my first digital health startup, but it’s my second as an entrepreneur. I started a consultancy back in 2007 that ran for about three years.
Xenia:

I’m Xenia Riasol, the Chief Operating Officer at nen. Before nen, I spent the last seven years of my career working in the Pharma industry. I worked at Almirall where I met Francesca. We were on the same team, where I was responsible for creating and deploying innovative digital solutions for patients, including Digital Therapeutics, across Europe. I’d call myself a digital strategy expert with a focus on commercialization models and global solution deployment. I also have an in-depth knowledge of the startup ecosystem because I worked closely with the startups that were part of the Digital Garden. I helped them manage and design their commercial models, find expansion opportunities, work with Pharma and so on. So while this is my first time as an entrepreneur, I have a good understanding of what it takes.
Prior to Pharma, I worked as a digital marketing and communication specialist at companies in the retail and food distribution sectors. I’m originally trained in the fields of advertising, PR and media studies. Over the years, I’ve specialized in digital business strategy and health specifically, and other things like eCommerce and digital marketing in general.
Randy:
Did you have a hard time convincing your parents that that was a real thing for a degree?
Xenia:
They have always been very open minded and supportive. Although it is true that they don’t always understand exactly what I’m doing in my day-to-day work, they believe in the purpose as much as I do. Different story with my 94-year old grandmother – she only gets that I work with a laptop!
Randy:
Where did the name nen come from?
Francesca:
nen is a nod to where the company was founded, in Barcelona, Spain. It means “kids” in Catalan. My ancestry is from Catalonia and Xenia is Catalan, so we thought it was a good name. We did a lot of research and discovered it’s pronounced almost identically in any country, so kids and parents won’t have trouble pronouncing it.
Randy:
It doesn’t mean anything bad in any language you know?
Francesca:
No it doesn’t. I also checked that.
Randy:
That’s great. Talk a little bit about nen and what problem it’s solving. Do you have a better mousetrap, or an entirely new one?
Francesca:
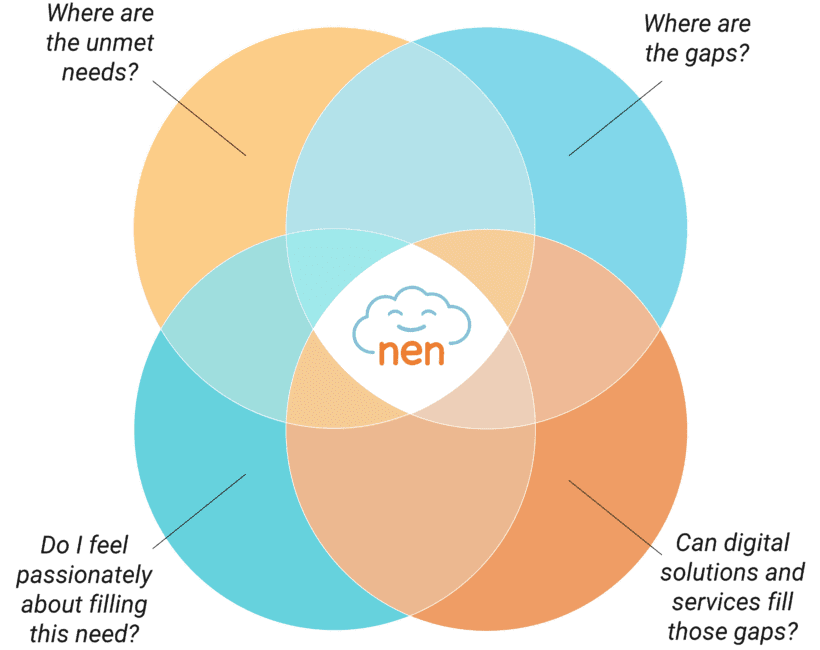
Well, we have a mousetrap, and we’re hoping it certainly adds benefits to kids and their families. In thinking about what I wanted to do after leaving Almirall, I sought something that would have an impact. Finding the right idea that we could be passionate about was tricky. So I put my consulting hat back on, landscaped the whole of the digital health market to find where there were gaps, and asked myself, can those gaps be filled by digital health solutions? Specifically Digital Therapeutics, because I really feel strongly that they’re the third wave of medicine. We’ve moved from small molecules and biologics, to cell and gene therapy, and then finally to Digital Therapeutics.
In my research, I was really surprised by the dearth of digital activity in pediatrics broadly, but specifically within the oncology space. Previously, we had worked on a Digital Therapeutic for pain. I was able to see how you could translate Cognitive Behavioral Therapy (CBT) in the management of adult pain with success. And I thought, well, why not apply this to kids?
So, we founded nen to help kids with cancer, their families and HCPs with pain management. nen offers a novel mission-driven approach to address pain management through play, leveraging gamification approaches and CBT to modulate pain and improve kids’ overall wellbeing and outcomes. We aim to create a Web-based platform for both smartphones and tablets. A gamified approach will assess, treat and offer continuous feedback to children based on their journey through the game. The modules will be age-appropriate, and designed to be engaging and enjoyable for kids.

When speaking to pain specialists, they were unanimous in that managing pain in pediatric oncology remains the highest unmet need for pain management. Almost 500,00 children will be diagnosed with cancer this year, and unfortunately, just about 100% of them will have pain at some point in their disease. nen will start with preschool aged children, from two to seven, that have the greatest unmet medical need and for whom it is the most difficult to assess and treat their pain. We will continue to develop our platform to serve patients from eight to twelve and then later for 13-17, for whom opioid sparing[1] remains a huge public health problem.
Once clinically validated for pediatric pain in oncology, we intend to run clinical trials in children with chronic pain to ascertain populations or subpopulations that could benefit from our platform. The oncology space is a little bit cleaner versus the chronic care space because these patients, from an experimental perspective, are far more controlled. We will largely be testing in an inpatient setting with the support and oversight of clinicians and nurses, who will ensure that our study is compliant with the protocol. Furthermore, because of the relative homogeneity of pain in cancer, we can design proof of concept clinical trials that will better represent an improvement as a result of our platform. Not only do we seek to resolve a huge unmet need in these kids and for these families, but we’re also taking the opportunity to show proof of efficacy in this environment.
Randy:
That’s really interesting. Frequently, when I talk to people who are in digital health and Digital Therapeutics especially, I ask, “How did you get into this?” And usually they say, “Well, this happened to me or someone in my family.” You really took an investor-oriented view of where the opportunity is in need, and just happened to land on something with a great human element to it.
Francesca:
Xenia and I are both really mission-driven. We’re looking to do what’s right for kids and their families. But we recognize that in order to get nen to that point where we can deliver it to kids and help democratize their pain management, we have to have an investable business. We have to create something that can get the appropriate investor backing in order to get us where we need to go.
Randy:
I’m curious, but if the data had come out that the number one money-making opportunity for you as a platform was a companion app for Botox, do you think you would’ve jumped on it?
Francesca:
No. While there were a lot of ideas that filled an unmet need, I didn’t feel passionately about them, so they were immediately discarded. My decision-making process was like a four-way Venn Diagram, if you will: Where are the unmet needs, where are the gaps, can digital solutions and services fill those gaps, and do I care?
Randy:
Startup founders may ask themselves, “How do I know if I want to co-founder with somebody? Do I have the right team?” How did you two arrive at doing this together? What’s your origin story?
Francesca:
I’m the founder of nen. When I had a vision of what it could be over the past summer, the only person I could imagine doing it with was Xenia. She and I worked together over the past three years. She took on a tremendous amount of responsibility and I admire her ability to learn and do things. She’s a perfectionist.
Xenia:
Thank you. As Francesca mentioned, we are mission-driven and dedicated. I was seeking the next step in my career, and I knew that I didn’t want to just be part of another big company working on something I wasn’t interested in. I was willing to change, to do something more hands-on, because sometimes you try to put yourself in things that don’t always go as expected. I really wanted to do something where I could have an impact. nen was the right decision for me. I was impressed with the proposition we were going to address and the value we would add. It was an immediate “yes” to join this adventure.
Randy:
Let’s talk a little bit about your stakeholder interviews. You identified pediatric oncology pain management as an area you could improve, and you wanted to drill down and talk to people working in it. How did you do your initial validation around the product concept? Is this an important enough problem and will somebody actually prescribe this and will someone take it?
Francesca:
While we are an early stage startup, Xenia and I draw from our extensive industry and more specifically digital health experience to accelerate our pace of maturity, and to leverage our network of experts to maximize our success as we build our platform and digital therapeutic solution. I was able to leverage my network from both the digital health world as well as from the investor community. In six months, I probably talked to 30-50 investors, healthcare practitioners, parents of kids with cancer and digital health gurus. The ideal molded a bit. There were things that definitely changed as a result of those conversations, like how to deploy the selling model, or how to focus on one very niche area, which frightens some of the investors. I would call people in my network and say, “Hey, I have this crazy idea. What do you think?” Some of them said, “It’s a crazy idea, stay in your job.” Others were encouraging enough that I decided to finally take the plunge, incorporate the business, quit my day job, bring Xenia on and do this full time.
Randy:
And what gave you that confidence that you really had a viable concept that checked all the boxes? Especially since there’s so much somebody in Digital Therapeutics has to sidestep.
Francesca:
The interest was there. Many people I talked to were supportive and propelled me on. Some people so much so that when I spoke with them, they’ve since looked into putting their own money into our SAFE, which I think is a pretty good validation of the concept.
Randy:
Could you elaborate more on what a SAFE is?
Francesca:
A SAFE is a Simple Agreement for Future Equity. Basically, you put money in now, then it converts into something valuable down the road, for instance, after a Series A. It’s actually not debt, because it doesn’t exist until the conversion point, if you will. We don’t have an equity structure as of yet because we don’t have a valuation yet. Plus, we haven’t laid out the whole framework. We’ll divy up the shares at our first valuation point. But until the SAFE converts, it doesn’t really exist. It’s an interesting way to bridge the investment path.
Randy:
It sounds like that to some extent, it requires an even higher degree of trust from investors than a traditional equity scheme: “I’m betting on you as a team. And I think you’ll get there.”
Francesca:
It really surprised me when I looked into it. I was a growth-stage investor; I didn’t invest in companies at this very early stage. So I wasn’t as familiar with SAFEs. I think they’ve taken on a bit of a life of their own over the past couple of years. It seems really startup friendly and really investor unfriendly, right? But the investors were the ones interested, telling me, “Hey, do this. I really want to be a part of it.” And they’re investing their own money, not on the behalf of an investment fund.
Randy:
It’s the ultimate in smart money, because it’s not just smart from the company. Somebody is personally taking their money out of their pocket, not their potential bonus ROI.
Francesca:
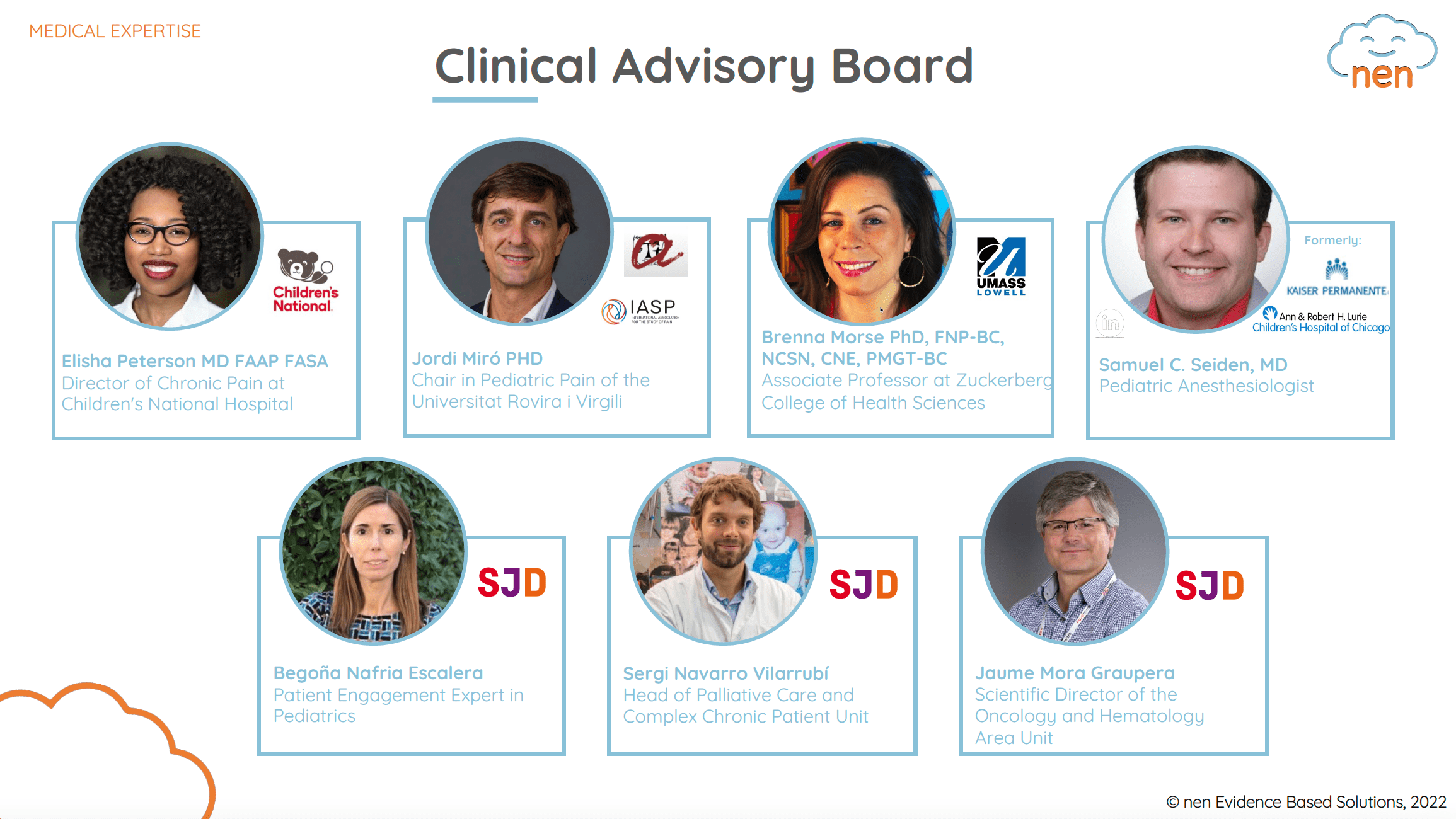
Exactly. And for us, we’re not doing it necessarily for the money, although the money will help to fund certain of our milestones. We’re doing it to build a cadre of advisors that have some skin in the game. We have a Clinical Advisory Board, which I’m sure we’ll go into more detail later. We have a Parents Forum that we can tap into to ask questions about the product and how to iterate on it. Now we’ve created a Business Advisory Board, made up of experts from the Digital Health ecosystem in the U.S. and EU.
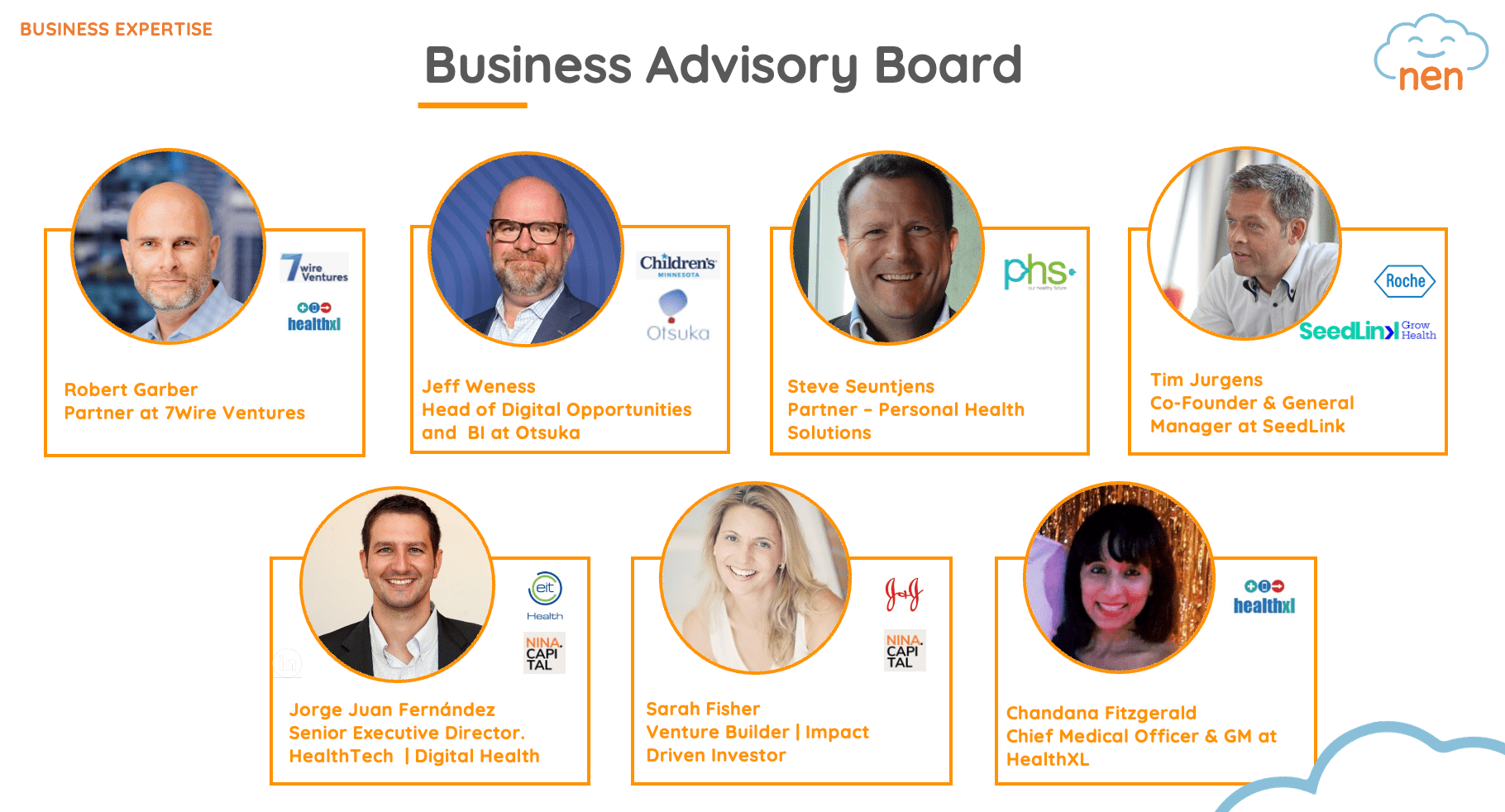
We are so fortunate to count this amazing group of digital health gurus among our Business Advisory Board, including digital health investors (Robert Garber, Steve Seuntjens and Tim Juergens), pediatric innovators (Jorge Juan Fernández and Jeff Weness), social impact drivers (Sarah Fisher) and digital health rainmakers (Chandana Fitzgerald). Their extensive experience will help guide us on our business model, commercialization and expansion plans and our funding roadmap. And these folks are for the large part those that had an interest in the SAFE, as well as some others outside of our Advisory Board.
Randy:
So you’ve got these killer advisory boards. How do you leverage them? Is it as a group or one on one? Do you have a Slack channel for each and you’re always in conversation, or are you calling up specific people for specific things? Do you ever get conflicting advice from them?
Xenia:
It depends on the role and the specific challenge we want to address, or the questions we want to ask. For the Clinical Advisory Board, we want to put everyone on the same page. But having them all together is not easy because of their schedules, as you can imagine. For the Business Advisory Board, we will try to do separate sessions depending on the area of expertise of each one.
We were talking today with one of our board members and he said, “Send me an invite every two weeks for 30 minutes. I want to be super updated on the topic.” Not everyone has that kind of time, and we will try to follow up with them on a monthly basis. But everyone is super keen on participating as much as possible. We are surprised about it as well.
Francesca:
It’s really surprising. What we did to find people for our Clinical Advisory Board was read the literature and call the names that kept coming up over and over again. We just called them, which you can do as a startup, and say, “Hey, this is what we were thinking. Could you help us?” And many of them said, “Sure!” We were like, “Oh! Great.”
Randy:
How do you get in touch with these world-class people and convince them of your Digital Therapeutic? Many of the people, I’m guessing, are at major medical centers and are thus hard to reach. You had to find a phone number, get through the department and administrator and all that just to hear them say, “Yeah, an app for oncology pain for kids. Sounds great!” What was that process like?
Francesca:
I honestly don’t know. It was a lot of luck. We gave them a very short blurb about what we were endeavoring to do. It resonated with them. They’re living and breathing this problem every day and looking for a solution to help these kids.
Our response rate was really high. We were hoping to have three to five. We ended up with seven and had to stop calling because we’re really happy with this group. It’s an impressive group of global experts in pediatric pain: Samuel C. Seiden, MD, a pediatric anesthesiologist who’s worked at several major U.S. children’s hospital; Sergi Navarro Vilarrubí, Head of the Palliative Care Service; Jaume Mora Graupera, oncologist leading the investigational unit; Begoña Nafría Escalera, Director of Patient Engagement and Pediatric Clinical Trials for a top European pediatric hospital; Elisha Peterson, MD MEd FAAP FASA, Director of Chronic Pain at Children’s National Hospital; Jordi Miro, PHD, Researcher and Pediatric Pain Psychologist; Brenna Morse, Registered Nurse/Ph.D. and contributor to current pain assessment scales. Brenna is also a lecturer at a major U.S. university that was on some of the early validation studies for the scales, so she knows this backwards and forwards. It’s a comprehensive, interdisciplinary team.
You asked earlier if sometimes we get conflicting advice. Sometimes we do, and then we have follow-ups with each of them because everyone’s super professional. If they do disagree, they’re not necessarily going to say so, but we really need to know how it really is in the clinic.
Xenia:
Many of these people are used to working with startups, have worked with at least one in their career lifetime, because most of them work in hospitals with accelerator programs. Or, they’re used to collaborating with other companies that bring innovation to the hospital. Supporting a startup isn’t new for them. It was actually new for me. Compared to other experiences I’ve had in my life, they were super open from the beginning – not only on the clinical part, but in the business area as well. The support we’re receiving is super impressive in that sense.
Randy:
I would also guess that they respond to both of your very engaging and extroverted personalities, and the fact that you’re coming to an area that has been very neglected and is mentally difficult to see (i.e., really sick kids) every day as a practitioner. They get the call from you and think, “This gives me a few minutes out of my day. What questions are they going to have now? It’s super interesting.” It’s a bit of an escape, in a good way.
Xenia:
We hope so.
Francesca:
Yeah, exactly.
Xenia:
You also asked why we came up with Digital Therapeutics as a solution. Because of our previous experience with DTx, I think we know how it works. We wanted to try it out with kids because 74% of children state that they prefer solutions presented in a technological platform.[2] What kids have access to now is basic and paper-based, which isn’t engaging for them at all. As for the therapeutic part, well, this population is very underserved. They don’t have this kind of support yet. Kids struggle to express their own pain to physicians and to their families, due to their age and due to a lack of a comprehensive approach or tools. We knew a Digital Therapeutic was the right solution.
Francesca:
It’s also a way to democratize care for all kids. Even in the most prestigious academic centers – there’s one that we’re working with that has 350 beds in their oncology unit, which is massive – they have just one pain psychologist. There’s no way that that pain psychologist can do 20 or 40 minutes of CBT with each kid every day. There aren’t enough hours in the day. But you hand them nen, and they can hopefully get the same level of care and manage their pain. Then, obviously, we can expand well beyond the medical centers.
Randy:
So it’s very scalable.
Francesca:
Very scalable. Once we’ve clinically validated it.
Randy:
I’ve talked to a couple of DTx founders lately. They’re adapting these existing therapies, but at the end of the day, there’s not even a fraction of the practitioners necessary if we continued with a service-based model to ever fill all the needs. So this is the only way.
Francesca:
We can talk about the business model and the progression later, but while we do need to build an investable business, we’re also very much driven to help as many kids as possible. There will always be a carveout to allow kids who can’t afford nen to have access to it.
Randy:
That’s great. I really see how nen was founded with vision and with heart.
Randy has even more questions for Francesca and Xenia in Part 2 of this interview. Learn about the current state of pediatric oncology care, the shape nen will take and lessons learned from both sides of the entrepreneur-investor relationship.
This is Part 1 of the two-part interview between Orthogonal’s Randy Horton and Francesca Wuttke and Xenia Riasol of nen.
Links to individual parts of the interview:
1. “Opioid Sparing” refers to the practice of combining a small dose of opioids with another pain relief medication that is non-addictive. 2. The Journal of Pain Volume 10, Issue 2, February 2009, Pages 173-179
Related Posts
Article
Top 10 SaMD Job Boards & Regional Organizations

Article
Top 10 SaMD Events, Conferences & Webinars

Article
Top 10 SaMD Publications, Blogs & Media

Article
Top 10 SaMD Communities, Organizations & Working Groups
